A Comprehensive Guide to the Menstrual Cycle
The below post is a culmination of several posts on what a conception. It has been strung together to create a one stop shop for a comprehensive look at the menstrual cycle.
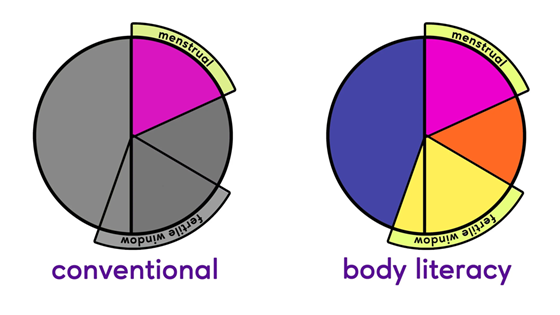
Building Cycle and Body Literacy
A menstrual cycle isn’t just a monthly inconvenience – it’s a dynamic interplay of hormones and organs that reflects overall health. In each cycle, your brain, ovaries, and uterus communicate to orchestrate events: the brain’s pituitary gland releases FSH (follicle-stimulating hormone) to mature ovarian follicles; growing follicles produce estrogen; a surge of LH (luteinizing hormone) then triggers ovulation[1][2]. This cascade of hormonal signals ensures the cycle progresses through its phases. Importantly, “menstrual cycle” does not just mean your period – it encompasses the entire sequence of changes from one period to the next[3]. In a healthy cycle, all phases (menstrual, follicular, ovulatory, luteal) play a role and give insight into your well-being[3].
Caption for image above: Conventional vs. body literacy perspectives on the menstrual cycle: A body-literate approach views all phases of the cycle (not only the period) as meaningful indicators of health.
One key to deep cycle literacy is recognizing that “normal” doesn’t equal 28 days for everyone. In fact, menstrual cycles normally range anywhere from about 24 up to 38 days in adult women[4]. Most people do not have textbook 28-day cycles, and slight variations cycle-to-cycle are common. For example, it’s typical for cycles to be a bit irregular during the teen years after menarche and again in the 40s approaching menopause[5]. Even in the 20s and 30s, few women have cycles that start exactly the same day each month. Thus, understanding your cycle means looking at your personal pattern over time, rather than comparing strictly to an average.
Another aspect of deeper cycle understanding is seeing your cycle as a vital sign of health (similar to heart rate or blood pressure). Health experts increasingly encourage viewing the menstrual cycle as a “fifth vital sign” because cycle patterns can reflect underlying health conditions[6]. Rather than just a reproductive event, your monthly cycle is a barometer of hormonal balance, metabolic health, and more. In short, developing cycle literacy means going beyond basics – appreciating how hormonal rhythms affect your body and using that knowledge to make informed health decisions[7]. Every phase of the cycle, not just your period, can tell you something about your health[3].
Your Cycle as a Vital Sign: What It Can Reflect About Your Health
Just as blood pressure or body temperature offers clues about health, your menstrual cycle provides a “monthly report card” for your body[8]. A well-regulated cycle often indicates that your hormones and organ systems are working in harmony. In fact, clinicians say the menstrual cycle reflects overall health status and should be considered an essential sign of health[6][9]. Regular cycles suggest balanced communication between the brain, ovaries, and uterus, whereas changes in cycle timing or symptoms can be early warning flags for issues.
What can your cycle tell you? If things are running smoothly, your periods usually come at fairly regular intervals – which might be monthly, but could be as short as ~21 days or as long as ~35–38 days depending on the individual[8][10]. The key is that they arrive in a predictable pattern for you. When your cycles start to shift significantly (for example, suddenly becoming much shorter, longer, or unusually heavy or painful), it can signal that something in your body may need attention[8]. For instance, late or missed periods, or very heavy periods, can be linked to health problems such as thyroid disorders, polycystic ovary syndrome (PCOS), excessive stress, or even anemia[11]. Rather than ignoring these signs, it’s wise to view them as your body’s communication. As one Harvard review put it, changes or ongoing problems with your cycle are clues that deserve investigation[9].
Viewing your cycle as a vital sign also empowers you to track it and share details with healthcare providers. Doctors actually encourage patients to monitor cycle patterns because it helps in diagnosing conditions early[9][12]. For example, consistently irregular cycles might prompt checking for hormonal imbalances or metabolic issues. By logging your periods (dates, flow, symptoms), you and your provider can gain valuable data. Cycle tracking is backed by science – research shows that monitoring your menstrual cycle can improve health management and doctor-patient communication[13]. It’s not just about fertility; it’s about overall wellness.
In summary, your menstrual cycle is not just a reproductive event isolated from the rest of your body. It’s intimately connected to other systems – metabolic, endocrine, even immune. Treating it like a vital sign means acknowledging that cycle irregularities or symptoms are as important to note as a fever or high blood pressure. A healthy cycle generally implies good hormonal balance, whereas cycle disturbances can be the first clue to conditions that might otherwise go unnoticed[14][12]. Pay attention to this important body rhythm, and don’t hesitate to discuss changes with a healthcare provider. It’s one of the most powerful feedback systems your body has.
Why Your Cycle Length Changes (Even When Nothing Feels “Wrong”)
It can be puzzling when you’ve had a fairly regular rhythm and then one cycle comes earlier or later than expected – especially if you feel perfectly fine otherwise. The truth is, menstrual cycle length can vary due to many subtle factors, even when “nothing feels wrong.” The most common culprit is hormonal fluctuations triggered by stress or lifestyle changes. You might not feel stressed, but your body could be responding to hidden stressors like travel, sleep disruptions, or workload changes. Emotional stress, physical stress (like intense exercise), or even nutritional stress (diet changes) can elevate cortisol and endorphin levels, which in turn interfere with the normal hormone signals for your cycle[15]. This is essentially your body’s way of saying, “Now might not be the best time for a pregnancy,” leading to ovulation being delayed or skipped. For example, a big project deadline or a minor illness one month might push your ovulation later, making that cycle longer.
Aside from stress, other lifestyle factors can cause an otherwise regular cycle to shift. Changes in body weight (either loss or gain), unusually intense exercise routines, or illness can all alter hormone levels and throw off your cycle timing[16]. Certain medications (like some antidepressants) or changing birth control methods can have temporary effects as well[16]. It’s also normal for cycle length to vary with life stages – in the first couple of years after menarche, cycles are often irregular, and as you approach perimenopause in your 40s, variability increases again[17][18]. Even if you’re in your prime reproductive years with a previously steady cycle, minor random anovulatory cycles (when no ovulation occurs) can happen on occasion, leading to an unusually long or short cycle for that month without any long-term issue.
In summary, a sudden change in cycle length isn’t usually a sign that something is terribly wrong – especially if it happens just once or infrequently. Our bodies are not machines; they respond to the environment. Research and clinical observations show that factors like stress, diet, exercise, weight, and sleep can all nudge the timing of ovulation and menstruation[16]. For instance, one month of higher stress might cause you to ovulate a bit late (lengthening the cycle), or vigorous marathon training could suppress ovulation altogether temporarily[15][19]. The important thing is pattern: if your cycle returns to normal the next time, it was likely a transient hiccup. However, if cycles continue to be highly irregular or accompanied by other symptoms, then it’s worth investigating. But one or two off-kilter cycles when life feels normal are generally just your body calibrating to subtle changes behind the scenes.
What “Regular” Actually Means When It Comes to Menstrual Cycles
Many people have heard that a “regular” cycle is 28 days, but in reality “regular” can encompass a broad range. Medical guidelines define a normal cycle length as anywhere from about 24 days up to 38 days for adult women[10]. So if your cycles are, say, usually 31 days or 26 days, that can still be perfectly regular – it’s regular for you. The key aspect of regularity is consistency: do your periods arrive at roughly equally spaced intervals? For example, one woman might have cycles that vary between 26 and 30 days; another might consistently be around 35 days. Both could consider their cycles regular, even though their average lengths differ. According to the U.S. Office on Women’s Health, you’re still regular if your periods usually come every 24–38 days – some women can even predict their period almost to the day, while others have a window of a few days variability, and both scenarios are considered normal[20].
In practical terms, a “regular cycle” means your period comes about the same time each cycle, without dramatic unpredictable swings. It’s normal for the timing to vary by a few days from month to month. In fact, research notes that it’s normal for a cycle to sometimes shift by up to 7–9 days and still be within the realm of regular[10]. So, for instance, if one cycle was 29 days and the next is 35 days, that could still be part of normal variability. What would count as irregular? Doctors often say that consistently having cycles shorter than ~21 days or longer than ~35–38 days, or variation of more than about a week between cycles, is irregular[21]. Also, if you have no idea when your period will come because the gap fluctuates wildly (like 25 days one month, 45 the next), that’s considered irregular.
The concept of regularity also ties to ovulation. Regular cycles typically imply that you are ovulating consistently, even if not on the exact same day each time. Meanwhile, very erratic cycles might indicate inconsistent ovulation. If you’re tracking your cycle, after a few months you can usually tell what’s regular for you[22]. Bottom line: Regular doesn’t mean a rigid 28-day cycle for everyone. It means a reliable pattern for your body, usually falling within a healthy range. If your cycle usually falls within that range and doesn’t suddenly change drastically, you can consider it regular[10]. Embracing this broader definition can be reassuring – you don’t have to fit an exact mold to be normal.
The Difference Between a Healthy Cycle and a Common One
It’s common for people to say “Oh, bad cramps are normal” or “It’s normal to feel miserable around your period.” But there’s a distinction between what is common (many people experience it) and what is healthy or normal from a medical standpoint. In a truly healthy cycle, symptoms like pain, mood swings, or very heavy bleeding should be mild to moderate and manageable. However, many people have come to accept severe symptoms as “just part of life” because they’re common. For example, having some cramps or fatigue with your period is very common, but pain so bad that you regularly miss work or school is not a normal healthy pattern – it could signal conditions like endometriosis or fibroids. As one OB/GYN aptly put it, “pain and discomfort being common…doesn’t always mean they are normal.” Menstruation shouldn’t mean suffering by default[23]. If you find yourself doubled over with cramps or unable to get out of bed due to fatigue or mood, that’s common for many, yes, but it’s a red flag that deserves attention.
A healthy cycle typically involves bleeding that lasts about 2–7 days, with total blood loss around 2 to 3 tablespoons (30–50 mL) – enough to require period products, but not soaking through a pad an hour for hours on end. It’s common for people to have heavier flow (especially in the first day or two), but soaking super tampons every hour or passing large clots is not healthy-normal; it might indicate fibroids or a clotting issue, for instance[11]. Similarly, some mood changes or irritability before your period can be common (we call it PMS), but extreme rage or depression every month isn’t healthy – it could be PMDD, a severe form of PMS that may require treatment. Many women have been told by well-meaning others that everything unpleasant is “normal.” As a result, issues like severe PMS or debilitating period pain often go untreated for years because they’re so common that people assume they must be normal.
To put it another way: “Common” means it happens often; “healthy/normal” means it’s expected and not a sign of dysfunction. Lots of people have PMS and cramps – common, yes. But the healthy version of PMS is more mild: perhaps you feel a bit moody or bloated, but you can carry on with life. Healthy cramps might mean you need a heating pad or an ibuprofen on day 1, but you’re not doubled over all day. When symptoms interfere with your daily life or well-being, that crosses into abnormal (even if your friends experience it too). For instance, very heavy or irregular periods are common in women with undiagnosed thyroid issues or PCOS – but once those conditions are treated, cycles often normalize. Heavy, painful, or irregular cycles can also lead to complications like anemia over time[11], so they shouldn’t be brushed off.
In summary, don’t confuse prevalence with normalcy. It’s common for people to report significant menstrual issues, but a healthy cycle is one where those issues are minimal. If you find yourself saying “My periods are awful, but that’s just how it is for everyone,” it might be worth re-evaluating. You might be in the “common but not normal” camp. Never hesitate to seek help for cycle problems just because they happen to a lot of people. Remember, menstruation shouldn’t mean misery[23]. Many period problems can be improved, so you can move closer to a healthy (and still common!) experience of what a menstrual cycle can be.
Why You Don’t Ovulate on Day 14 (and Why That’s Normal)
There’s a pervasive myth that every woman ovulates on Day 14 of her cycle. In reality, ovulation timing is highly variable from person to person and even from cycle to cycle. The “Day 14” idea comes from the average of a 28-day cycle, where ovulation roughly mid-cycle is common. But consider this: in a study of over 800 women with 28-day cycles, only 14% ovulated on day 14 exactly[24]! In that study, ovulation timing ranged anywhere from day 11 to day 20 in women who all had 28-day total cycle lengths[24]. That’s a huge range, and these were “regular” cycles – just not clockwork 14th-day ovulation. So if you don’t ovulate precisely at mid-cycle, you are absolutely not alone.
Every person’s hormone trajectory is a bit different. Some have a shorter follicular phase (the first part of the cycle before ovulation), causing ovulation to happen earlier (say day 11 or 12). Others have a longer follicular phase, perhaps ovulating on day 19 or 20, even though the total cycle length might still fall in normal range. It’s also normal for the same woman to ovulate on, for example, day 16 one month and day 14 the next. Cycle regularity doesn’t require ovulating on an exact day, just that the overall length is fairly consistent for you. In fact, studies show nearly half of all women’s cycles vary by 7 days or more in length[24], which means the timing of ovulation likely shifts accordingly.
Additionally, not everyone’s luteal phase (time after ovulation) is exactly 14 days – though 12-14 days is typical, it can be a bit shorter or longer, which also affects which day ovulation falls on. For instance, a woman with a consistent 10-day luteal phase who has 28-day cycles would ovulate around day 18 (later than “day 14”), which might be completely normal for her.
The bottom line: Ovulation is not a fixed date on the calendar; it’s an event that occurs when a dominant follicle in the ovary has matured enough to release an egg. That timing can vary due to stress, illness, travel, or just normal variation in follicle development. Even in textbook “regular” cycles, a one-size-fits-all Day 14 ovulation is a myth[24]. So if you’re tracking fertility and notice you ovulate on day 12 or day 20, rest assured that’s normal for you. The key is understanding your own pattern rather than the mythic average. After all, normal ranges are averages and approximations – nature thrives on a bit of variability.
Hormones & How You Feel
(This section explores how hormonal fluctuations across the menstrual cycle influence mood, energy, and overall feelings. Many people notice changes in focus, sociability, and emotions at different times – here’s why.)
Why You Feel More Social, Focused, or Energized at Certain Times of Your Cycle
Ever notice there are days when you feel on top of the world – outgoing, confident, mentally sharp – and other days when you’d rather hibernate? Much of this can be traced to where you are in your cycle. As estrogen rises during the follicular phase, especially approaching ovulation, it has energizing and mood-lifting effects. In the roughly week or so after your period and leading up to ovulation, many women report feeling more optimistic, social, and focused. Biologically, higher estrogen is associated with increased serotonin and dopamine activity in the brain, which can improve mood and cognitive function. Clinically, doctors observe that in the mid-cycle phase, patients often have more energy and even “increased confidence or motivation,” as one OB/GYN noted[25][26]. You might find you’re more inclined to make plans, tackle big projects, or be physically active during this time. Some refer to this as the “inner summer” of your cycle – you’re at your peak in terms of sociability and vigor.
Around ovulation, when estrogen hits its peak and there’s also a small surge in testosterone, many experience a boost in libido and social confidence. It’s not uncommon to feel more attractive or communicative at this time (an evolutionary nudge, since this is when fertility is highest). In fact, research and anecdotal reports suggest ovulation can bring a subtle shift toward being more outgoing – sometimes called the “flirty” phase. Kaiser Permanente’s women’s health experts note that during ovulation, women often feel “more confident” and “more social,” driven by those hormonal peaks[26]. You might find those are the days you volunteer to give a presentation or go to a networking event, almost naturally timed by your body.
On the flip side, after ovulation in the luteal phase, progesterone rises and estrogen falls, which for many has a calming or even sedating effect. You may notice a shift toward being more reflective or introverted in the week or so before your period. It’s not that you lose your social skills, but the high-energy spark might dim a bit. This is the time when you might prefer a cozy night in to a big social gathering. It’s perfectly normal – your brain chemistry is essentially winding down from the ovulatory high. Some women actually report feeling very focused on nesting or detail-oriented tasks during part of the luteal phase (sometimes called the “inner autumn”), even as they become less interested in socializing.
In summary, these changes in sociability and energy are driven by hormonal rhythms. Estrogen (especially when peaking pre-ovulation) tends to correlate with feeling more energized, outgoing, and mentally sharp, while progesterone (dominant after ovulation) can bring a quieter, calmer mood. Neither is “good” or “bad” – it’s a natural ebb and flow. By noticing this pattern, you can plan around it: schedule that big meeting or party during your high-estrogen days if you can, and give yourself permission for more low-key self-care days when you know you’ll be in your quieter phase. Your cycle is effectively tuning your brain and body in different ways throughout the month[27][26].
The Science Behind Cycle-Related Mood Changes
Many people experience mood shifts over their cycle – maybe feeling bluesy or irritable before the period, or extra upbeat mid-cycle. The science behind these emotional ebbs and flows boils down to hormones interacting with brain chemistry. During the luteal phase (after ovulation), levels of estrogen and progesterone initially run high and then drop sharply right before menstruation. This hormonal rollercoaster can significantly affect neurotransmitters like serotonin, which is a key player in mood regulation. In some individuals, the normal drop in estrogen late in the cycle is linked to a drop in serotonin availability in the brain[28]. Serotonin is often dubbed the “feel-good” chemical – it helps maintain a positive mood, among other things. If serotonin levels fall, you might experience classic PMS mood symptoms: sadness, irritability, anxiety, or mood swings.
In fact, PMS (premenstrual syndrome) is essentially the result of your body’s response to the hormone changes of the menstrual cycle[29]. Not everyone’s brain reacts the same way – this is why some people have very mild PMS and others have more severe mood changes. Studies indicate that some women are more serotonin-sensitive: as estrogen drops and progesterone metabolites rise, their serotonin levels fluctuate more dramatically, leading to pronounced symptoms[28]. Progesterone itself, through its breakdown product allopregnanolone, interacts with GABA receptors in the brain (which influence calm vs. anxiety). For women who experience PMS, one theory is that these brain receptors respond differently to the hormone changes, causing discomfort rather than calm.
To put it simply, right after ovulation, estrogen and progesterone are high – some women feel great during this time, while others might already start to feel a little emotionally “off” if they’re sensitive. Then, about a week or so before your period, both estrogen and progesterone start declining if no pregnancy occurred. It’s this decrease – essentially a form of hormonal withdrawal – that can trigger mood changes. The symptoms can include irritability, a shorter fuse, feelings of sadness, or anxiety. It’s notable that conditions like PMDD (Premenstrual Dysphoric Disorder), a severe form of PMS, are thought to involve an exaggerated drop in serotonin in response to normal hormone shifts[30]. In PMDD, women suffer serious depression or anxiety in that luteal-to-menstrual transition, and medical treatments often involve SSRIs (antidepressants that boost serotonin) or hormonal therapies to stabilize levels[30].
On the flip side, when your period starts and in the early follicular phase, hormones are at their lowest. Some people actually feel an emotional lift once bleeding begins, as if the tension breaks – possibly because the hormonal turmoil of the late luteal phase has resolved with the drop. Others might still feel low energy or mood during menstruation due to prostaglandins (chemicals causing cramps and inflammation) or simply the physical toll of bleeding.
In summary, the science of cycle mood changes centers on hormone-driven shifts in brain chemicals: estrogen and progesterone influence serotonin, GABA, and other neurotransmitters. As they rise and fall, especially the falls, your brain chemistry adjusts, and you feel those changes as mood or energy alterations[28]. Understanding this can be validating – you’re not imagining it, and you’re not alone. It also means there are strategies to cope, from lifestyle tweaks (exercise can boost serotonin, for example) to medical options if needed. Your cycle is a chemical conversation with your brain each month, and mood changes are one way we “hear” that conversation.
Estrogen vs. Progesterone: How Hormonal Shifts Affect Energy, Sleep, and Appetite
Estrogen and progesterone are the two superstar hormones of the menstrual cycle, and they have quite different personalities – which you likely feel in terms of your energy, sleep quality, and even hunger levels. In the first half of the cycle (follicular phase), estrogen is dominant and steadily rising. Estrogen is like an energizer: when it’s higher and steadier, many women find they have more energy and even require slightly less sleep to feel good. Estrogen can help keep body temperature slightly lower and is associated with more restorative sleep in some studies (it’s one reason women’s sleep can worsen after menopause when estrogen falls)[31]. On the energy front, as estrogen climbs, it tends to make you feel more mentally alert and physically capable, which corresponds to that feeling of being more active or focused in the pre-ovulation phase. It also has an appetite-suppressing effect – when estrogen levels are high and stable, appetite is often easier to manage, and cravings are less intense[32]. This is why in the week after your period, you might notice you’re not as ravenous and you might even have to remind yourself to eat at times. Your brain’s hunger centers are getting a signal that you’re satiated, partly thanks to estrogen.
Progesterone, on the other hand, takes center stage after ovulation (in the luteal phase). Progesterone is often described as having a calming or sedating effect – it can make some women feel more mellow or sleepy. In fact, progesterone rises your core body temperature slightly, which is one reason some women experience a bit of insomnia or restless sleep in the late luteal phase; the body likes cooler temperatures for deep sleep, and that shift can disrupt things for some[33]. On the flip side, progesterone can also make some women feel sleepy especially earlier in the luteal phase – it’s sometimes called the “natural Valium” for its calming qualities. So you might notice you’re sleepier than usual or have a harder time waking up in the morning during the week before your period. If estrogen is the get-up-and-go hormone, progesterone is the take-it-easy hormone. It’s no surprise some women don’t hit personal record times in their workouts in the luteal phase – energy might be a tad lower.
When it comes to appetite, progesterone is the main culprit behind those infamous pre-period cravings. As soon as ovulation passes and progesterone starts climbing, many experience increased appetite and stronger cravings, especially for carbs or sweets[34]. Biologically, your body is preparing just in case you got pregnant – it doesn’t “know” if you did or not yet – so it tends to make you hungrier to encourage more calorie intake. Evolutionarily, this would help support an early pregnancy. Even in controlled studies, women eat more calories per day on average in the luteal phase than the follicular. You might notice you’re suddenly snacking more or that a previously resistible cookie is now calling your name loudly. Hunger cues often ramp up when estrogen dips and progesterone rules[32][35]. Many women also feel more bloated or puffy in the progesterone phase – progesterone can cause you to retain some water (hence that pre-period bloating and breast tenderness). It’s also responsible for slightly slowing down digestion (hello, constipation or just feeling sluggish gut-wise before your period).
In a nutshell, estrogen tends to rev you up – better mood, higher energy, dampened appetite, and solid sleep (up to a point) – whereas progesterone tends to slow you down – a bit more fatigue or relaxation, increased appetite and cravings, and changes in sleep (for some, sleepiness, for others, restless sleep)[31][34]. Both hormones are crucial, and their effects can vary person to person. The important thing is recognizing these patterns in yourself. That way, you don’t panic when you have a week of insatiable hunger or a couple nights of poor sleep – you can attribute it to where you are in the cycle and respond accordingly (for example, prioritize a bit more rest or allow an extra healthy snack). It’s another facet of body literacy: knowing that your hormones are not just about reproduction – they affect your whole body, including how energetic you feel, how well you snooze, and when you raid the fridge.
Why PMS Happens: A Hormone and Brain Chemistry Perspective
PMS (Premenstrual Syndrome) is practically a household term – referring to the constellation of symptoms (mood swings, irritability, anxiety, bloating, etc.) that occur in that week or two before your period. But why does PMS happen? From a biological standpoint, PMS is caused by the normal hormone swings of the cycle interacting with your brain chemistry[29]. After ovulation, when the body is gearing up for a possible pregnancy, estrogen and progesterone levels soar. Then, if no pregnancy occurs, these hormone levels plummet sharply in the late luteal phase (usually a few days before your period). This rise and fall, especially the fall of estrogen and progesterone, triggers PMS symptoms in susceptible individuals[30]. The drop in estrogen can cause lower levels of serotonin (which, as mentioned earlier, is key for mood regulation and feeling good). Meanwhile, changing progesterone levels (and its byproducts) affect GABA receptors in the brain, which are involved in calming anxiety – some women experience an overreaction to this influence, leading to feelings of anxiety or irritability.
Think of it this way: throughout the cycle, your body and brain adjust to a certain level of hormones. When those hormones take a nose-dive right before menstruation, it’s akin to a mini withdrawal that your brain registers. Decreasing levels of estrogen and progesterone after ovulation and before menstruation are the main triggers for PMS symptoms[30]. This hormone drop can lead to fluid retention (hence bloating), changes in glucose metabolism (hence sugar cravings), and notably changes in neurotransmitters. Serotonin in particular may drop alongside estrogen – and serotonin regulates mood, sleep, and appetite[36]. Lower serotonin can mean moodiness, sadness, or trouble sleeping. Additionally, progesterone’s metabolite allopregnanolone normally has a calming effect via GABA; in women with PMS or PMDD, some research suggests their brains might suddenly become less sensitive or even adverse to allopregnanolone as it rises and falls, creating anxiety instead of calm. This is an active area of research as scientists try to pinpoint why some get PMS and others don’t.
From an evolutionary perspective, there isn’t a clear benefit to PMS – it might just be a side effect of the complex hormonal dance. Some have theorized it could signal to a woman that she didn’t conceive this cycle (thus perhaps triggering certain behaviors), but that’s speculative. What we do know is up to 75% of women report some PMS symptoms, while about 20-30% have symptoms significant enough to affect daily life, and about 5-8% have PMDD which is severe[37]. Common PMS symptoms like mood swings, irritability, fatigue, and physical symptoms (breast tenderness, bloating, headaches) all tie back to those hormone shifts. For example, breast soreness happens because high progesterone in luteal phase causes fluid retention in breasts; then it eases once period starts and hormones drop.
In summary, PMS happens because your brain and body respond to the cyclic hormone changes – particularly the pre-period hormone nosedive[38]. It’s a mix of hormonal and neurochemical changes. That’s why approaches to easing PMS often involve either smoothing out those hormonal fluctuations (like using birth control to prevent the big fall in hormones) or targeting neurotransmitters (like using SSRIs to boost serotonin in the luteal phase). Understanding that PMS has a real physiological basis (not “in your head” in the dismissive sense) can be validating. It also underscores that if PMS is really interfering with your life, it’s worth talking to a healthcare provider – because it’s rooted in biochemistry that can often be helped.
How Stress Shows Up in Your Cycle (Even When Life Feels “Manageable”)
You might be handling everything life throws at you with grace – meeting deadlines, caring for family, even fitting in exercise – and think, “I’m a little stressed, but I’m fine.” Then your period is late or acts unusual, and you wonder why. Stress is one of the most powerful external factors that can alter your menstrual cycle, even when you don’t subjectively feel “stressed out.” The body’s stress response system (the adrenal glands pumping out cortisol and adrenalines) interacts directly with the reproductive hormone axis. When you experience stress – be it emotional, physical, or even nutritional (like strict dieting) – your brain may alter how it releases GnRH (the hormone that kickstarts each cycle), which can delay or suppress ovulation[15]. In evolutionary terms, it’s a protective mechanism: during times of high stress or hardship, the body might postpone reproduction. This is why, for example, chronic stress can lead to missed periods or very irregular cycles. Even if you feel like you’re coping, your body might be saying “let’s hold off on ovulation this month until things stabilize.”
Stress doesn’t have to be extreme like a trauma; everyday manageable stress can add up in the body’s accounting. Maybe you started an intense workout program, or you’re not sleeping enough due to work – those are physical stresses. Your body might respond by tweaking your cycle timing. It’s been observed that even events like traveling across time zones (disrupting your routine and sleep) or studying for exams can shift the cycle that month. Cortisol, the primary stress hormone, can interfere with the normal rise of estrogen and the LH surge needed for ovulation[39][40]. In some cases, you might still ovulate but a bit later than usual – hence a longer cycle. In other cases of acute stress, you might skip ovulation entirely (an anovulatory cycle), resulting in either a missed period or a very odd, breakthrough bleeding at some point.
One OB/GYN explained that any stress – “emotional, nutritional, or physical” – can cause increased endorphins and cortisol that interrupt hormone production, leading to an abnormal cycle[15]. For example, women who lose a significant amount of weight or have a very low BMI often see their periods stop (because the body perceives insufficient resources to support a pregnancy). That’s a form of physiological stress. Runners or athletes who suddenly up their training mileage may find their cycles become irregular – the body interprets intense exercise as stress too. Even positive life changes, like planning a wedding or moving to a new house, can stress the system enough to delay a period by a few days.
It’s also fascinating that sometimes stress-induced cycle changes happen not immediately, but a cycle or two later. The body might “power through” during the stressful event and only afterward, when you think all is well, does the cycle hiccup. This can make it hard to connect the dots. For instance, a really stressful month at work might result in a weird period the next month.
Recognizing stress in your cycle can be as simple (and frustrating) as noticing, “Huh, I was a week late and I’m not pregnant. Oh yeah, last month was crazy at work.” If you find irregular cycles and stress correlate, it’s a sign to incorporate more stress reduction techniques (exercise, meditation, therapy, better sleep). Often, when the stressor resolves or you adapt, cycles resume their normal pattern – studies show that a high percentage of women recover normal periods once stress or weight issues are addressed[41].
In summary, stress commonly “shows up” in the menstrual cycle as delayed or missed ovulation, resulting in late or missed periods[42]. It can also cause heavier periods or more cramps (since stress can increase inflammation and prostaglandins, possibly making cramps worse). Even if you feel you’re managing, your body might be absorbing that stress and prioritizing survival over reproduction in subtle ways. So, if your cycle is acting funky and you’ve ruled out pregnancy, consider the stress factor. It’s your body’s gentle (or not-so-gentle) reminder to slow down and take care of yourself. Often, by listening and adjusting, you’ll see your cycle return to its regularly scheduled programming in a month or two.
Cycle Tracking & Body Signals
(This section focuses on understanding the signs your body gives you throughout the cycle – and how to track them in a balanced way. By observing things like temperature, cervical mucus, etc., you can learn a lot, but it’s important not to let tracking become an obsession.)
Cycle Tracking Without Obsession: How to Use Data Without Overinterpreting It
Tracking your menstrual cycle – recording periods, ovulation signs, symptoms – can be incredibly empowering. It’s a core part of body literacy, helping you predict fertile days or simply understand your patterns. However, there’s a fine line between attentive tracking and obsessing over every tiny blip. To use cycle data in a healthy way, focus on long-term patterns rather than day-to-day fluctuations. For example, taking your temperature each morning (for basal body temperature, BBT) is useful to confirm ovulation occurred, but one weird temperature reading on a bad night’s sleep shouldn’t send you into a panic. It’s the sustained shift over several days that matters, not a single number. Similarly, noticing cervical mucus is great, but don’t stress if one day it seems off – it can be affected by temporary factors like hydration or mild infections.
One strategy is to track consistently but with self-compassion. If you forget to chart one day or your data looks messy due to travel or illness, just continue the next day – missing one data point isn’t the end of the world[43]. In fact, fertility educators emphasize consistency over perfection. It’s a common mistake to get frustrated and give up if you miss a day or if the signs confuse you; instead, just keep observing and the picture will clear over time[43][44]. Patience is crucial. It often takes a few cycles to really see your unique rhythm, so there’s no need to interpret one odd cycle as a crisis.
Another tip: use multiple signals to cross-check, so you don’t overinterpret one sign. For instance, if you’re charting BBT and it’s all over the place (maybe due to stress or inconsistent sleep), pay attention to your cervical mucus or ovulation test kits that cycle. Combining methods (temperature + mucus, for example) gives a more reliable picture. Planned Parenthood notes that tracking another sign like cervical mucus can be really helpful if your temperature chart gets messed up because you were sick or stressed. In other words, having more than one metric prevents you from obsessing on one data point that might be an outlier.
It’s also helpful to remember why you’re tracking. If you’re trying to conceive, yes you want to catch that fertile window, but stressing can actually inhibit conception. If you’re tracking for health insights, you want to notice meaningful changes, not drive yourself crazy with every minor deviation. Think of tracking like keeping a journal: look for recurring themes and big-picture trends. A single “off” day or even an “off” cycle can be noted and then let go. If it becomes a pattern (e.g., luteal phase consistently shortening or ovulation getting significantly delayed every cycle), then it’s actionable information to possibly discuss with a doctor.
Avoiding obsession also means setting boundaries. Maybe you record your data in the morning and then don’t think about it the rest of the day. If you find yourself checking your tracker app five times a day, or feeling anxious, give yourself permission to take a break. Remember, the goal of cycle tracking is to empower you, not to add stress. If it’s becoming stress-inducing, scale back. You might skip tracking during a vacation, for instance, to just let yourself live in the moment.
In summary, use cycle data as a helpful tool, not an anxiety meter. Trust your body – it’s resilient and one quirk doesn’t mean it’s broken. By charting consistently and focusing on patterns over time, you’ll gain valuable insights without falling down a rabbit hole of overinterpretation. As one fertility educator put it, “Don’t expect a perfect cycle right away…be patient with yourself”[44]. With that mindset, you can appreciate what your body signals are telling you, while still keeping your peace of mind.
What Basal Body Temperature Really Tells You (and What It Doesn’t)
Basal Body Temperature (BBT) – your temperature first thing in the morning before you even get out of bed – is a cornerstone of many fertility awareness methods. Here’s what it’s great for: confirming that ovulation has occurred. After ovulation, the hormone progesterone rises, and one of progesterone’s effects is to elevate your resting body temperature slightly. So you’ll typically see your BBT chart low-ish temperatures in the first part of the cycle, then a noticeable sustained jump (often around 0.4°F or 0.2°C or more) after ovulation, which stays higher until your next period. If you see about 3+ days of higher temps, you can be fairly confident ovulation happened just before the first high temp. This is valuable for understanding your cycle’s timing – you can count your luteal phase length, know that you did ovulate, etc.[45].
However, here’s what BBT doesn’t do well: predicting ovulation before it happens. BBT is a retroactive sign of ovulation[46]. By the time your temperature rises, the ovulation event (release of the egg) has already passed – usually by a day or so. This means BBT alone isn’t very useful for preventing pregnancy (because once it rises, you’re mostly past the fertile window) or for pinpointing the fertile days in advance if you’re trying to conceive. It more tells you “Yep, looks like I ovulated on Tuesday” after the fact. To predict ovulation, other signs like cervical mucus or LH ovulation predictor kits are needed, because BBT will always lag behind.
Another limitation: BBT can be influenced by factors unrelated to your cycle. If you have a fever, if you drank alcohol the night before, if you jumped out of bed and ran around before taking it, or even if you had a very poor night’s sleep or slept in a cold vs. hot room – all these can skew a morning reading. One erratic temperature doesn’t mean you didn’t ovulate or something is wrong; it might mean you need to discard that data point as noise. That’s why in fertility awareness, we often look for a pattern of at least three elevated temps above the previous six or so temps – to smooth out any one-day anomalies.
What BBT really tells you: it tells you that progesterone is in your system (hence ovulation occurred, since only after ovulation do you get a corpus luteum making progesterone)[45]. It also can give insight into your luteal phase length (from ovulation day to last day of high temps). For instance, if you notice your temperature rises but then drops and your period comes just 8 days later, that might suggest a short luteal phase, which could be relevant if trying to conceive. If you conceive, your temps will stay elevated beyond the usual luteal span (this is one early clue some charters use to suspect pregnancy).
What BBT doesn’t tell you: it can’t pinpoint the exact moment or even day of ovulation with certainty – you infer ovulation occurred maybe the day before the temp shift, but the BBT itself is just an indirect marker. It also doesn’t tell you anything about egg quality, follicle health, or fertility issues apart from ovulation timing. And as mentioned, it won’t give you advance warning of ovulation in the current cycle[46]. If you are looking for your fertile window, BBT alone will always tell you a bit too late.
In practice, many people use BBT charting combined with other cues (like cervical mucus checks) for a fuller picture. The strength of BBT is its objectivity – it’s a number, whereas something like judging mucus can feel subjective. Seeing that clear biphasic (two-level) chart is reassuring evidence your body did what it was supposed to. If you never see a temp shift, it might indicate an anovulatory cycle for that month.
To use BBT effectively: take it at the same time each morning before any activity, after at least a few hours of sleep. Log it faithfully, but don’t freak out over one off-number. Look at the trend. When you see that sustained rise, mark ovulation (often you mark ovulation day as the last low temp before the rise). Know its limits – treat BBT as your cycle’s rearview mirror, not a crystal ball.
In short, BBT really tells you whether and when you likely ovulated, but it doesn’t predict ovulation and can be thrown off by external factors[46]. It’s a wonderful tool for confirming patterns but should be combined with other signs if you need to identify fertile days ahead of time. Understanding this will prevent disappointment or confusion in using temperature as part of your cycle tracking toolkit.
Cervical Mucus Explained: What Changes Mean and Why They Matter
Cervical mucus (the fluid or discharge you notice throughout your cycle) might not be something you gave much thought to until you started learning about fertility, but it’s an incredibly useful body signal. The cervix produces mucus in response to hormonal changes, and its consistency and amount change in a predictable way through the cycle[47]. Here’s the typical pattern for someone with a roughly average cycle:
Right after your period: you often have a few “dry” days with little to no discharge[48]. Early in the cycle, estrogen is still low, so the cervix isn’t producing much mucus yet. These days, if they occur, are typically not fertile.
As estrogen starts rising (before ovulation): the cervix responds by making more mucus. At first this mucus may appear thick, sticky, or tacky – kind of white or yellowish and paste-like[49]. You might notice it as a tacky residue. This happens as an egg is developing in the ovary and estrogen levels climb. These days (often lasting around 3-5 days) indicate you’re approaching fertility, but the mucus is not yet optimal for sperm. It’s like a heads-up that ovulation is on the horizon[49].
Right around ovulation (estrogen peak): mucus transforms into what’s often described as “egg white” cervical mucus (EWCM)[50]. This is the most fertile type. It becomes clear, slippery, and stretchable – you could stretch it between your fingers an inch or more in a raw-egg-white-like string. It also often gives a lubricative sensation. Many women feel wetness in their vulva on these days. This fertile mucus typically lasts about 2-4 days leading up to and including ovulation[50]. Why does it matter? Because sperm need this type of mucus to survive and swim. Fertile EWCM nourishes sperm and helps transport them through the cervix into the uterus. Without fertile mucus, sperm would die off much quicker in the vagina’s naturally acidic environment. So, those “slippery” days are your peak fertile days – the time when intercourse (if trying to conceive) is most likely to lead to pregnancy[50]. From a contraceptive standpoint, those are the “unsafe” days to have unprotected sex if you’re avoiding pregnancy.
After ovulation (when progesterone rises): the character of mucus changes rather abruptly. Progesterone causes mucus to become thick and scant again – often described as cloudy and sticky or it may disappear, leading to dry days[51]. Essentially, after ovulation, the body’s focus is on potentially nurturing an embryo, so cervical mucus forms more of a plug to prevent additional sperm or bacteria from entering. You’ll likely notice that the wet, lubricative sensation is gone a day after ovulation. Many experience a quick switch back to feeling dry or only having minimal, thicker discharge for the rest of the luteal phase (about 11-14 days long)[51].
Then the cycle repeats with the next period and the whole pattern resets.
Why these changes matter: Beyond indicating fertile vs non-fertile days, cervical mucus is a window into your hormonal status. If you never observe fertile-quality mucus, it could mean your estrogen is not peaking normally (anovulatory cycles, or other issues). If you see mucus patterns but irregularly, it might reflect hormonal ups and downs (sometimes PCOS causes multiple patches of mucus as the body attempts ovulation multiple times).
For those trying to conceive, tracking cervical mucus is one of the best ways to time intercourse. The appearance of fertile, egg-white mucus is essentially a big neon sign that says “Ovulation imminent – now’s the time!” And since sperm can live up to 5 days in fertile mucus[52], having sex when you first notice fertile mucus means sperm will be waiting when the egg is released. Studies have shown cervical mucus status is highly correlated with actual fertile window timing – often more so than calendar calculations.
For those avoiding pregnancy naturally, cervical mucus tracking (the Billings or ovulation method) is a proven method when done correctly. You abstain or use protection during any days of fertile-type mucus and a couple days after.
It’s also worth noting how amazing our body’s design is: the cervix, under estrogen’s influence, opens up and secretes this hospitable mucus for sperm, effectively creating channels that guide sperm in. Then under progesterone, the cervix closes and mucus becomes impenetrable, like a natural gatekeeper.
To check cervical mucus, you can wipe with toilet paper before peeing each time and note sensations (dry vs. slippery) and look at the mucus on the paper (or your fingers) – over time, you get an eye for the categories. As with all things, individual variation exists: some women have tons of mucus, others have just enough to notice. If you have difficulty observing, a specialist can help with techniques. Certain factors (like dehydration, antihistamines, breastfeeding, etc.) can reduce mucus.
In summary, cervical mucus goes from “nothing”, to sticky, to slippery, back to sticky/none in a cycle[47][50]. These changes are key to fertility – the slippery “egg-white” days are when pregnancy is possible (and also when you might feel different down there). Paying attention to mucus can tell you when you’re fertile, when you’ve likely ovulated (once it dries up), and even clues about hormone health. It’s one of those body signals that once you tune into, you wonder how you ever ignored it!
Why One “Off” Cycle Doesn’t Mean Something Is Wrong
It’s easy to get worried when you have an unusual cycle – maybe your period came 10 days late, or you skipped a month, or it was much heavier or lighter than normal. But in the vast majority of cases, one “off” cycle is not a cause for alarm. Our bodies are not clockwork, and many factors can cause a temporary blip. As a certified nurse-midwife succinctly put it: “One irregular period every now and then isn’t something to be overly concerned about.”[53]. If your cycles are usually in a normal pattern and you experience a one-time weird cycle, chances are it’s a fleeting disturbance – perhaps due to stress, travel, illness, or just random variation – and things will return to usual shortly.
Common scenarios might include: suddenly a cycle is much shorter (maybe you ovulated earlier than usual) or much longer (you ovulated late or not at all that cycle). Or your period was markedly lighter one month (could be an anovulatory cycle, where often the subsequent bleed is lighter because no strong hormone build-up occurred) or much heavier once (maybe a late ovulation led to a thicker uterine lining that shed more). While these experiences can be unsettling, a single occurrence can fall within normal variability. Most women will experience at least one irregular or unusual period at some point, even if generally regular[54].
The body often self-corrects. For instance, if stress delayed your ovulation and made one cycle 50 days long, you might find the next cycle is a bit shorter than your norm as your body gets back on schedule. Or if you skipped a period (again common under stress or sometimes randomly), the next one might be heavier or come a bit unpredictably. This doesn’t immediately signal a chronic problem.
Healthcare providers typically say they become concerned only if irregularities persist. If cycles are “consistently inconsistent,” then it’s worth a check-up[53]. But one or two odd cycles are usually considered within the range of normal occurrence. Another example: in your early 40s, it’s common to start having an off cycle here or there due to perimenopausal hormonal changes – again, not alarming as a one-off, but part of a transition that eventually becomes a pattern.
So, when confronted with an off cycle, the best approach is: take note of it, but don’t panic. If you track, you can jot down any potential factors (e.g., “period late – was under a lot of stress at work this month”). Often, the explanation becomes clear in hindsight. If the next few cycles go back to normal, you can generally shrug that one off as an outlier. However, if irregular cycles repeat or other symptoms come up (like persistent heavy bleeding, severe pain, etc.), then it’s time to investigate further.
To reassure yourself, remember that even things like slight thyroid fluctuations or a transient illness can throw off a cycle. Our hormones are part of a complex feedback loop easily influenced by overall health. One irregular period could simply mean your body was busy fighting a cold or dealing with a chaotic month and decided to postpone ovulation.
Medical consensus echoes this calm stance: Had one irregular period? Don't stress just yet[55]. Give it a little time. As that midwife said, occasional irregularity isn’t typically worrisome[53]. So, unless you have reason to suspect something like pregnancy or a specific condition, the advisable response to one rogue cycle is usually watchful waiting. Chances are, you’ll be right back on track soon.
How Long It Takes to Learn Your Cycle Patterns (and Why Patience Matters)
When you first start paying close attention to your cycle – perhaps tracking signs like temperature or mucus, or just noting your moods and symptoms – it’s natural to hope you’ll “figure it out” in one month. But learning your unique cycle patterns is more of a marathon than a sprint. Generally, it takes a few cycles – often around 3 to 6 months – to really start seeing your patterns clearly and to trust them. That’s because any given single cycle can have quirks. It’s only by observing multiple cycles that you can distinguish the usual from the unusual. As one fertility educator advises, “It’s important to have patience… Don’t expect immediate results or a perfect cycle right away.”[44]. Our bodies aren’t robots, and learning their language takes some time.
The first cycle you chart or monitor might feel confusing: Is that temperature shift really ovulation? Is my PMS always this bad, or was this month unique? After two or three cycles, you might notice, for example, “Ah, I typically ovulate around day 15, except that one stressful month it was day 20.” Or “I see a pattern that I get a headache on the first day of my period consistently.” These insights crystallize over time.
Patience matters for a few reasons:
Cycle lengths can vary: You might have a 27-day cycle one month and a 30-day the next. If you assumed from one cycle that you’ll always be 27 days, the next cycle might throw you off. After a few cycles, you’ll know your range (maybe you usually vary between 27-30 days, for example).
Biological variation: Ovulation can naturally fluctuate by a couple of days cycle-to-cycle. It’s only by observing multiple cycles that you can say, for instance, “My luteal phase (post-ovulation phase) is consistently 13 days long, even if ovulation day varies a bit.”
Data Interpretation: If you’re using methods like the fertility awareness method, you improve in interpreting your signs after some practice. The first month checking cervical mucus, you might be unsure what is “eggwhite” mucus versus just wetter. But give it two or three months and you’ll become much more confident in identifying your fertile mucus. Similarly, with temperature charting, it might take a couple cycles to get the hang of taking it at the right time and seeing the biphasic pattern clearly.
There’s also an emotional aspect. Initially, it’s easy to get frustrated if you can’t decipher everything immediately. But trust that your body has cycles within cycles, and a clearer picture emerges with time. One month you might have more pronounced ovulation symptoms (like mittelschmerz pain or high libido), another month they might be subtle. Only by noting across several cycles can you say, “Usually, I feel ovulation pain about half the time,” etc.
From a medical perspective, when investigating something like possible luteal phase defect or irregular cycles, doctors often ask for records of about 3 cycles minimum, because any single cycle can be an outlier. For example, if you suspect you have a short luteal phase, confirming it over 3 cycles is more reliable than just one possibly weird cycle.
If you’re coming off hormonal contraception, it might take a couple cycles for your natural rhythm to show up – another reason patience matters.
The payoff for patience is big. After several months, you’ll likely feel far more attuned to your body’s signals. You’ll start to predict, “I bet my period will start tomorrow or the next day,” based on that familiar pattern you’ve observed. Or you’ll realize that the mood dip you get on day 25 always resolves once your period starts, which can be reassuring when you’re in it.
In conclusion, give yourself at least 3 cycles of consistent tracking or observation to really learn your patterns, and even more if possible[44]. Each cycle will teach you something new, and over time the puzzle pieces will form a cohesive picture of your cycle. Patience is truly a virtue here – your body operates on its own timetable, and by observing it calmly over months, you build a reliable understanding that one could never get from a single snapshot. Remember: cyclical means repetitive – the patterns will reveal themselves through repetition. Hang in there, and by a half-dozen cycles, you’ll likely feel like a cycle detective who’s cracked her case.
Science of Ovulation & Timing
(In this section, we delve into the mechanics and timing of ovulation – clarifying what ovulation really is, why its timing isn’t set in stone, and what the body is doing before and after this pivotal event.)
Ovulation Is an Event, Not a Date: Understanding Biological Timing
We often speak of ovulation as if it’s a scheduled date (“Day 14,” as discussed earlier, or any specific day). But in reality, ovulation is a one-time event in the cycle – the moment when an egg is released from the ovary – and it doesn’t always adhere to a calendar date. Biologically, ovulation occurs once a dominant follicle in the ovary reaches maturity and responds to a surge of luteinizing hormone (LH). Think of it as a process culminating in a singular event, similar to how a graduation happens on a day but only after weeks of preparation. Leading up to ovulation, follicles in the ovaries have been growing for days (or even weeks), and the body has been ramping up estrogen. Only when the estrogen level peaks does it trigger that LH surge from the brain’s pituitary gland, which then causes ovulation about 24-36 hours later[56].
So, rather than a preset date, ovulation is timed by your body’s readiness. This means if conditions aren’t right (say you’re sick or stressed), your body might postpone that LH surge, delaying ovulation. Alternatively, if you had a particularly robust follicle developing quickly, you might ovulate a bit earlier in a given cycle. It’s helpful to view ovulation like a ripening fruit – it will drop when it’s ripe, not strictly on day X.
Also, ovulation itself is a brief event – the follicle ruptures and releases the egg, which is then viable for maybe 12-24 hours at most[57]. This is why we say the fertile window (when pregnancy can occur) is the few days before ovulation plus the day of ovulation – because sperm need to be around when that short window opens. In fact, the egg is optimally fertilized within the first 12 hours or so after release; beyond 24 hours unfertilized, it’s no longer viable. So ovulation is not a phase that lasts days – it’s a point in time. The “ovulatory phase” usually refers to the day or two around ovulation, but the egg release itself is over in moments.
Understanding this can shift how you approach tracking: instead of thinking “I ovulate on CD15 usually,” it might be better to think “I tend to ovulate around the middle of my cycle, when my body is ready.” In a given cycle, ovulation might happen at 9am or 9pm on whatever day – we don’t usually know the hour (unless monitored by ultrasound), but we see the signs after the fact (temperature rise, etc.). It’s quite literally an event that can occur at any time on ovulation day.
Additionally, ovulation is not guaranteed to alternate ovaries each cycle or anything that rigid. It’s often random which ovary ovulates (the one with the most ready follicle steps up)[58]. So that too is not a fixed pattern.
Why does it help to view ovulation as an event? Because it underscores flexibility. If you’re trying to conceive, you realize you need to aim for the days leading up to that event (since once it’s passed, the chance is largely gone). If you’re avoiding, you realize you must be cautious in the lead-up because once ovulation “happens” the window closes quickly. Also, it highlights that the timing can shift cycle to cycle – it’s not locked to a date. One cycle’s stress can push the event later; another cycle’s early follicle growth spurt can bring it forward.
From a biological timing perspective: typically, once the body commits to ovulation (with the LH surge), it’s fairly predictable – ovulation will occur about 10-12 hours after LH peaks[57]. That’s why ovulation predictor kits give you a heads up about 24 hours in advance of the event (they detect LH). The entire ovulatory process (follicle rupture, egg pickup by the fallopian tube) happens quickly, and then the luteal clock starts.
In summary, ovulation is not a standing appointment on day 14 for everyone; it’s an event driven by physiology and it can only be broadly predicted by understanding your own cycle cues. Embracing that it’s an event will make sense of why some cycles you ovulate sooner or later. It’s your body deciding the timing internally, not the date on the calendar. As a result, be open to variability and watch your body’s signs – they’ll tell you when the event is nearing and when it’s done, more reliably than a pre-marked calendar can.
Why Ovulation Timing Can Shift Month to Month
If you’ve tracked your ovulation over several months, you might have noticed it doesn’t always happen on exactly the same cycle day. Maybe one month you ovulated on day 13, another on day 17. This month-to-month variability in ovulation timing is completely normal. The primary reason lies in the part of the cycle called the follicular phase – the phase before ovulation when follicles are developing in the ovaries. The follicular phase is somewhat open-ended in length. Of the two main cycle phases, the follicular phase is the one that varies the most in length from cycle to cycle for an individual woman[59]. It can be influenced by both internal factors (like hormone levels, ovarian response) and external factors (stress, illness, etc.). In contrast, the luteal phase after ovulation is usually more consistent in a given woman (often about 12-14 days). So if something causes a delay in when a follicle matures, your ovulation day will shift, and thus total cycle length shifts.
Here are some specific reasons ovulation timing can move around:
Stress and lifestyle: As mentioned, stress can delay ovulation. If your body perceives stress around the time it would normally ovulate, the brain might temporarily put the brakes on the LH surge. Ovulation is then postponed until stress hormones recede. Travel, acute illness, heavy exercise, or emotional turmoil in the first half of the cycle can all potentially push ovulation later than usual. Once that stress passes, the follicle can resume growing and ovulation occurs.
Variation in follicle recruitment: Each cycle, a cohort of follicles in the ovaries begins to develop. It’s somewhat random how quickly one will become dominant. In some cycles, one follicle may gain dominance early and reach maturity sooner. In other cycles, it might be slower, or the first chosen follicle might falter and another takes over (which can cause a delay). This natural variation means you won’t ovulate the same day every time.
Aging and hormonal changes: As women get older, cycles often shorten a bit (follicular phase can shorten because follicles get recruited faster due to lower egg supply – paradoxically making ovulation earlier). But in perimenopause, ovulation can become irregular or delayed often. Even in your 20s/30s, minor hormonal fluctuations cycle-to-cycle (like differences in FSH levels or estrogen feedback) can slightly speed up or slow down the process.
Health conditions or disruptions: If you have something like a thyroid imbalance or polycystic ovary syndrome (PCOS), ovulation might naturally be more irregular. Treating those conditions can stabilize ovulation timing. But even a simple thing like coming off birth control or emergency contraception can cause a one-time delay or irregular ovulation as your body resets.
No two cycles are identical: The body is responsive to environment and internal rhythms. Ovulation timing can even differ seasonally for some women or after major life events. There’s also some evidence that in the first cycle or two after childbirth (when cycles return) or after a miscarriage, ovulation might be a bit off-schedule initially.
Importantly, having some variation is not only normal, but expected. For example, one large study illustrated that even women who typically have 28-30 day cycles might occasionally have a much shorter or longer cycle at random. Follicular phase length can vary and thus ovulation “day” can shift[59]. If someone usually ovulates day 14 but one month ovulates day 20 due to stress, that cycle might be ~34 days long instead of 28 – a one-time change.
When should one be concerned? If ovulation becomes very erratic or absent frequently, that’s when to look deeper (could be signs of conditions like PCOS or other endocrine issues). But slight shifts (a few days here or there) are usually benign.
To adapt to this reality: if avoiding pregnancy, don’t assume you’re safe just because you think you “always” ovulate on a certain day – build in a buffer because it can surprise you. If trying to conceive, don’t only have intercourse on one calculated day; watch your signs (like cervical mucus) because your body will cue you if ovulation is early or late compared to the norm.
In short, ovulation timing is not etched in stone – it can change with circumstances, age, and randomness. That variability is a normal part of reproductive life. The menstrual cycle is considered a dynamic system, not a static one, so understanding and respecting that flexibility will save you from worry when it happens and help you manage fertility with more nuance.
What Happens in Your Body Before Ovulation (A Hormone Timeline)
The lead-up to ovulation is a carefully orchestrated hormone saga. Let’s walk through the timeline of what’s happening in your body in the days leading up to the egg’s release:
Cycle Day 1 (First day of period): This marks the beginning of the follicular phase. Your estrogen and progesterone levels are low (they plunged at the end of the last cycle, triggering menstruation). Low hormones signal the brain that it’s time to start a new cycle. The pituitary gland (a small gland at the base of your brain) responds by sending out follicle-stimulating hormone (FSH) in slightly increased amounts[1]. FSH’s job is to “wake up” a batch of ovarian follicles (each containing an egg) to start developing. Early in this phase, as your period ends, you might have several small follicles growing.
Follicle development and rising estrogen: Among the recruited follicles, one will usually start to pull ahead as the dominant follicle. This follicle secretes estrogen – so as it grows, your estrogen levels climb. Estrogen has a few jobs now: it helps the uterine lining (endometrium) rebuild after your period, and it also affects the cervical mucus (making it progressively more fertile-friendly). Importantly, the increasing estrogen provides feedback to your brain. For most of the follicular phase, rising estrogen actually tamps down FSH output (preventing too many follicles from maturing) and keeps LH low. But it’s building up to a key switch.
About 5-7 days before ovulation: One follicle is usually clearly dominant by now and estrogen is climbing steeply. You might notice cervical mucus appearing now – first sticky, then creamy.
A day or two before ovulation (the estrogen peak): That dominant follicle is nearing maturity and pumping out a high level of estradiol (estrogen). When estrogen reaches a threshold level, it flips the switch in the brain from negative feedback to positive feedback. This is a pivotal moment: instead of suppressing gonadotropins, high estrogen now tells the pituitary to release a surge of LH (luteinizing hormone)[56]. This is the famous “LH surge”. Along with LH, there’s a smaller bump in FSH too[60]. The LH surge is essentially the trigger for ovulation – it initiates final maturation of the egg and weakens the follicle wall.
Ovulation (the main event): About 24-36 hours after LH begins to surge, ovulation occurs. The follicle bursts and releases the egg. The egg is swept into the fallopian tube. LH levels peak roughly 12 hours before the egg actually comes out[56]. Ovulation typically happens ~10-12 hours after the LH peak[57]. So if you had a way to pinpoint your LH peak to, say, 8am on a given day, ovulation might occur that evening. Leading up to ovulation, you might feel a twinge or cramp on one side (mittelschmerz) – that’s the follicle stretching the ovary’s surface[61].
Immediately after ovulation: The now-empty follicle in the ovary transforms into the corpus luteum – a little progesterone factory. Within a day or so after ovulation, progesterone levels start rising (and estrogen dips slightly then continues at a moderate level). This marks the start of the luteal phase.
Let’s recap the hormone timeline succinctly: FSH rises early to recruit follicles[1]; estrogen rises throughout the follicular phase as the dominant follicle grows[1]; when estrogen hits a high peak, it triggers the LH surge[59]; LH surge causes ovulation ~24-36 hours later[56]; then progesterone rises after ovulation.
During all this, your body gives external hints: as estrogen climbs, you see fertile cervical mucus and perhaps heightened libido. When LH surges, some ovulation predictor kits can detect that in urine giving you a positive result (typically ~1 day before ovulation). Ovulation itself you might only know happened in hindsight by signs like basal temp rise or the fact that fertile mucus dries up.
It’s amazing how coordinated it is: the brain and ovaries communicating via hormones to pick the best egg and release it at the opportune time. However, if anything in that timeline goes awry – say estrogen doesn’t reach a high enough peak, then LH surge might not happen and ovulation could be delayed or skipped. But in a normal cycle, the sequence is FSH up -> follicle/estrogen up -> LH surge -> ovulation, each step enabling the next[1][2].
Understanding this timeline helps you know, for example, why you see egg-white mucus 2 days before ovulation (because estrogen is at its max then), or why ovulation predictor kits need to be timed in that window (to catch LH surge shortly before ovulation).
The Luteal Phase Explained: What Your Body Is Doing After Ovulation
Once ovulation has occurred, your cycle enters the luteal phase – a more even-keeled, planned-out stage typically lasting about 12-14 days (though anywhere from 11 to 16 days can be normal for individuals). The luteal phase is named after the corpus luteum, which is the “yellow body” that the ovarian follicle turns into after releasing the egg. Think of the corpus luteum as a temporary endocrine gland that’s now on progesterone-production duty. It secretes increasing quantities of progesterone, and also some estrogen, to prepare the body for possible pregnancy[62].
Here’s what’s happening in the luteal phase:
Progesterone’s role: Progesterone is aptly named (“pro-gestation”) because it’s all about making the uterus hospitable for an embryo. Under progesterone’s influence, the uterine lining (endometrium) changes from the proliferative state (it built up under estrogen) to a secretory state[63]. This means the glands in the endometrium start secreting nutrients and the lining becomes more lush and spongy, ready for implantation of a fertilized egg. Progesterone also causes your basal body temperature to increase slightly right after ovulation[64], which is why we see that thermal shift in charting. This temperature will stay elevated throughout the luteal phase because progesterone remains high[64].
Cervical changes: Progesterone causes the cervical mucus to thicken and form a sort of plug[65]. This is protective – it makes it difficult for any new sperm (or bacteria) to get through the cervix, essentially “closing the gate” after the fertile window. That’s why after ovulation, you typically go dry or only have thick, non-fertile mucus; the fertile watery mucus is gone until next cycle.
Systemic effects: Progesterone can have various effects – it often leads to slightly heightened metabolic rate (hence higher temps, and sometimes why you might feel hungrier in luteal phase), it relaxes smooth muscles (sometimes causing slight constipation or bloating), and it can cause breast changes (many women experience swollen, tender breasts in the luteal phase, because progesterone dilates breast ducts and causes some fluid retention[66]). Also, both estrogen and progesterone are high in luteal, which together can cause the notorious PMS symptoms in some, especially as they drop at the end.
Luteal phase consistency: Unlike the variable follicular phase, your luteal phase length is usually consistent for you (give or take a day). The corpus luteum has a set lifespan – if no pregnancy occurs, it’s programmed to function about 14 days, then regress. When the corpus luteum regresses (dies), it stops making progesterone and estrogen, and the abrupt withdrawal of those hormones causes the uterine lining to break down – cue your period, and back to Day 1.
If pregnancy occurs: If the egg was fertilized and implants, the developing embryo will produce hCG (human chorionic gonadotropin) around a week after ovulation, which “rescues” the corpus luteum and tells it to keep producing progesterone[67]. The corpus luteum will then continue making progesterone for the first trimester until the placenta takes over. That high progesterone prevents a period from happening – which is why a missed period is a key early pregnancy sign.
Think of the luteal phase as the “work” phase where your body either nurtures an early pregnancy or prepares to reset. During this time, the corpus luteum is doing a lot: maintaining the uterine lining and keeping conditions suitable[62]. Progesterone peaks around the middle of the luteal phase then starts falling if no pregnancy.
If you’re tracking symptoms, the luteal phase is typically when PMS symptoms might appear, especially in the final 3-5 days as progesterone and estrogen start to decline if you’re not pregnant. The drop in hormones can cause mood changes, and progesterone’s earlier effects can cause things like bloating or breast tenderness.
Key point: the luteal phase is remarkably stable for most individuals. For example, someone might always have a 13-day luteal phase. So if you know when you ovulated, you can often predict when your next period will come by adding your luteal length. If your luteal phase is shorter than ~10 days consistently, that might be an issue for sustaining pregnancy (called luteal phase defect), but a day or two of variation can happen.
In summary, after ovulation, your body shifts into progesterone mode: the uterine lining is being nurtured, cervical mucus thickens, body temperature rises, and your whole system sort of holds its breath waiting to see if implantation will occur. When it doesn’t, the corpus luteum folds, hormone support withdraws, and that triggers menstruation – thus completing the cycle and readying the next one[67]. The luteal phase is the “second act” of the cycle, often overlooked, but it’s vitally important for reproduction and also significantly influences how you feel in that post-ovulation timeframe.
How Hormones Communicate Across Systems (Brain, Ovaries, Uterus)
The menstrual cycle is a beautiful example of inter-system communication in the body – mainly between the brain, the ovaries, and the uterus, but it truly involves the whole body (which is why you can feel cycle effects in mood, energy, etc.). Let’s break down the main players and their “conversation”:
Hypothalamus & Pituitary (Brain): It all starts in the brain. A part of your brain called the hypothalamus secretes GnRH (gonadotropin-releasing hormone) in pulses. This hormone travels a short distance to the pituitary gland (also in the brain), telling it to release FSH (follicle-stimulating hormone) and LH (luteinizing hormone) – together called gonadotropins. Think of GnRH as the boss giving orders, and FSH/LH as the managers carrying them out. FSH and LH then enter the bloodstream and head to the ovaries.
Ovaries: The ovaries receive FSH and LH signals and respond by adjusting their production of estrogen and progesterone, and by maturing eggs. For example, when the pituitary sends FSH, the ovaries say “Roger that, we’ll stimulate some follicles.” Those follicles grow and produce estrogen. As follicles get bigger, estrogen output increases – that estrogen travels through the bloodstream back to various parts of the body (uterus, brain, etc.). When estrogen reaches a high level, the ovaries in essence signal the brain (“Follicle ready!”) – how? That high estrogen flips the feedback to cause the LH surge from the pituitary. So the ovaries talk back to the brain via hormone levels. LH then triggers ovulation in the ovary. After ovulation, the ovary (through the corpus luteum) produces a lot of progesterone (and some estrogen).
Uterus: The uterus is a target organ responding to ovarian hormones. It’s not sending signals back in the form of major hormones, but it definitely is part of the loop in that if pregnancy occurs in the uterus, signals will then be sent (hCG from the implanted embryo) to rescue the ovary’s corpus luteum. But during the cycle, the uterus is like the stage being prepared. Estrogen from the ovaries tells the uterine lining, “Grow and proliferate!” The uterus thickens the endometrium accordingly. Then progesterone from the post-ovulation ovary tells the uterus, “Okay, now secrete nutrients and get ready for possible implantation”[63]. If implantation doesn’t happen, hormone levels fall and the uterus sheds the lining (your period). If implantation does happen, the embryo (in the uterus) produces hCG which communicates back to the ovary (corpus luteum) to keep making progesterone[67], and it may also have systemic effects like nausea.
Whole-body communication: These hormones don’t only affect the reproductive organs. They travel system-wide, which is why you have brain effects (mood changes via neurotransmitters), metabolic effects (temperature, hunger changes), breast changes (tenderness due to ducts responding to hormones)[66], etc. In essence, the menstrual hormones are in constant cross-talk with various body systems – an interplay of endocrine (hormonal), nervous, and reproductive systems. For example, the brain’s mood center responds to ovarian hormones (hence PMS mood swings), and the brain’s thermoregulatory center responds to progesterone (hence BBT rise).
A good way to visualize the hormonal communication is as a feedback loop: The brain (hypothalamus/pituitary) sends FSH/LH to ovaries; the ovaries send estrogen/progesterone signals back to the brain to let it know how follicles are developing[68]. The brain adjusts output accordingly (e.g., when high estrogen is detected, it triggers LH surge). Meanwhile, the ovaries’ hormones communicate with the uterus to prepare or reset the lining, and if the uterus (via an embryo) needs to communicate back (via hCG), it will.
It truly is an integrated axis often referred to as the HPO axis (hypothalamic-pituitary-ovarian axis). Changes in one part of this axis can affect the others. For instance, if the thyroid (another endocrine gland) is underactive, it can disrupt GnRH pulses in the brain and mess up the whole conversation, leading to irregular cycles. Or stress hormones (cortisol) can interfere with GnRH, delaying ovulation – that’s like static on the line in the brain-ovary phone call.
One could say the brain, ovaries, and uterus work together as a team, with constant feedback, to keep the cycle running smoothly[68]. If something’s off – say the ovaries aren’t producing enough estrogen because a follicle isn’t developing well – the brain may not trigger an LH surge, so ovulation won’t happen and the uterus won’t get the progesterone message to enter luteal phase properly. Each part depends on the others doing their job.
The emerging scientific understanding even considers the menstrual cycle a “vital sign” because it reflects how well these body systems are communicating[68]. A regular cycle means the brain, ovaries, uterus, and endocrine system are in sync. An irregular cycle might mean one part of the chain isn’t responding normally.
In short, hormones serve as the messengers between the brain, ovaries, and uterus – coordinating the timing of egg release and preparation of the uterine environment[68]. This hormonal dialogue happens constantly and ensures that all systems are on the same page for potential reproduction. It’s a remarkable symphony of signals: truly, your cycle is the result of multiple organ systems communicating in concert to protect your health and potential fertility. Each period you have is a sign that this cross-talk occurred – even if no pregnancy happened, the cycle is a sign your body had a successful round of internal communication.
Understanding this interplay not only is fascinating but also emphasizes why overall health (stress, nutrition, etc.) can impact your cycle – because those factors can influence the brain or hormone levels, which then ripple through the whole system. Keeping the lines of communication clear (through a healthy lifestyle) helps keep your cycle humming along as the integrated network it is.
Sources:
Harvard T.H. Chan School – Menstrual Cycle as a Vital Sign[68][10]
Adriatica Women’s Health – Irregular Menstruation Q&A[53]
Clearblue – Fertility Myths[24]
Cleveland Clinic – PMDD Causes[30]
Fertility Awareness Project – BBT is a retroactive sign[46]
LearnBodyLiteracy – Body Literacy perspective[3]
[1] [2] [4] [5] [52] [57] [58] [59] [60] [61] [62] [63] [64] [65] [66] [67] Menstrual Cycle - Women's Health Issues - Merck Manual Consumer Version
[3] [7] What Is Body Literacy? — Learn Body Literacy
https://www.learnbodyliteracy.com/what-is-body-literacy
[6] Menstrual Cycles as a Fifth Vital Sign | NICHD - Eunice Kennedy Shriver National Institute of Child Health and Human Development
https://www.nichd.nih.gov/about/org/od/directors_corner/prev_updates/menstrual-cycles
[8] [9] [10] [11] [12] [13] [14] [68] How Menstrual Cycles Shed Light on Overall Health | Harvard T.H. Chan School of Public Health
https://hsph.harvard.edu/mahalingaiah-lab/news/how-menstrual-cycles-shed-light-on-overall-health/
[15] [19] [41] [42] How Stress Affects Your Menstrual Cycle | UT Physicians
https://www.utphysicians.com/how-stress-can-affect-your-menstrual-cycle/
[16] [17] [18] [21] Sudden Change in Menstrual Cycle Length
https://www.verywellhealth.com/sudden-change-in-menstrual-cycle-length-7483332
[20] [22] [56] Your menstrual cycle
https://womenshealth.gov/menstrual-cycle/your-menstrual-cycle
[23] What does a healthy period feel like? - Flourish
https://blog.prismahealth.org/what-does-a-healthy-period-feel-like/
[24] Popular Myths and Facts About Getting Pregnant – Clearblue
https://www.clearblue.com/fertility/myths-and-facts
[25] [26] [27] 4 phases of the menstrual cycle: How to feel your best around your period | Kaiser Permanente
[28] [29] [69] Understanding PMS and Your Cycle | UMass Memorial Health
https://www.ummhealth.org/health-library/understanding-pms-and-your-cycle
[30] [36] [37] [38] Premenstrual Dysphoric Disorder (PMDD): Causes & Treatment
https://my.clevelandclinic.org/health/diseases/9132-premenstrual-dysphoric-disorder-pmdd
[31] Women’s Hormones Impacting Sleep | VPFW
https://vpfw.com/blog/how-womens-hormones-can-affect-their-sleep-and-tips-for-improving-it/
[32] [34] [35] Estrogen, Progesterone, and Testosterone: How Hormones Affect Appetite, Fat Storage, and Muscle (and Your Weight Loss Results) – Women's Health Center of Chicago
[33] Understanding Cycle Syncing
[39] How Cortisol Affects Women's Health and the Menstrual Cycle
https://www.nesaz.com/how-cortisol-affects-womens-health-and-the-menstrual-cycle/
[40] The Link Between Stress and Your Periods - Women's Health Services
https://www.womenshealthservices.com/blog/the-link-between-stress-and-your-periods
[43] [44] [45] [46] Avoid these mistakes when you're learning Fertility Awareness — Fertility Awareness Project
https://fertilityawarenessproject.ca/blog/learning-fertility-awareness
[47] [48] [49] [50] [51] What is the Cervical Mucus Method? | Cycle, Stages & Chart
[53] Ask A Midwife: Irregular menstruation - Adriatica Women's Health
https://adriaticawomenshealth.com/ask-a-midwife-irregular-menstruation/
[54] Irregular Periods | Northside Gynaecology | Kedron & North Lakes
https://www.northsidegynaecology.com.au/conditions/irregular-periods/
[55] When your period decides to extend its visit a little longer than usual ...